
How the Israeli data used to sell COVID vaccine efficacy exposed its own lies
The "Real World Data" used to prop up the vaccine efficacy narrative shoots itself in the foot


Now that we have pretty much demolished the authenticity of the Pfizer trial1 and that only the most clueless propagandists still dare to use it to defend the argument of vaccine effectiveness, the argument has - predictably - shifted to “real world data”.
“Real world data” essentially means all those observational studies used to prop up the original COVID vaccine trial data (which nobody really believes any more).
The “real world data” became the new Grail of scientific evidence used by governments and institutions to quash any dissent in the ranks when those of us, who knew that the original studies weren’t kosher, tried to speak up. The dogma went something like this:
“We can believe the original Pfizer vaccine study because multiple studies, for instance out of Israel, are showing that the vaccine effectiveness is about 95% in real world data”
The reality of course was telling us something very different to “the vaccine prevents 95% of infections” (as covered by Arkmedic in a previous article2). In actual fact COVID cases (and deaths) went up after the vaccine rollout, when they should have disappeared if the advertised claim was true.

More recently Jikkyleaks, trying to explain to Professor Jeffrey Morris that his latest study didn’t correlate at all with reality, had one of those ideas which made the mouse famouse3: comparing infection rates by arms in Israel among 4 different “real world data” studies, studying various samples of the same population through time.
The result posted was this graph:

The Israeli studies were instrumental in defending the idea that the trial efficacy was “as advertised” - and that the only reason we would later observe a decline in effectiveness was the variants. These studies were all published in the infamous NEJM :
Dagan et al., 2021, published on February 4, 20214, which was looking at the period from December 20, 2020, to February 1, 2021, on unvaccinated versus at least one dose.
Bar-On et al., 2021, published on September 15, 20215, was evaluating the period from July 30 to August 31, 2021, on 2 doses versus 3 doses.
Bar-On et al., 2022, published on April 5, 20226, was evaluating the period from January 10 to March 2, 2022, on 3 doses versus 4 doses.
Magen et al., 2022, published on April 13, 20227, was evaluating the period from January 3 to February 18, 2022, on 3 doses versus 4 doses.
The principle was simple: every time a product version started to be intensively advertised by the media and political apparatus, a study was published, proving how the product was working well in Israel, transformed by Benjamin Netanyahu in what was presented as the equivalent of a country-scale clinical trial8.
For the sake of the argument here, we’ll assume that the effectiveness for the product advertised is a complete fabrication, and only look at the raw infection rate among the “control group” used in the study.
The hypothesis here being that, for each extra dose being investigated, the “control group” that had fewer doses (but were vaccinated) should - if the vaccines worked - have lower rates of infection then those pesky “unvaccinated” which the world’s paid leaders disparaged so viciously over the last 4 years.
The alternative hypothesis of course is that the vaccines didn’t work at all (to prevent infection as claimed) and the claimed effectiveness was merely a result of shifting vaccinated cases into the unvaccinated group or some other nefarious “shell game” trick.

So let’s see which it is - starting with the first and most influential paper of Dagan in 2021.
Dagan 2021 features, on its Figure 2, this comparison between unvaccinated and vaccinated individuals:

The infection rates of documented SARS-CoV2 infection aren’t provided, but we can compute the person‑days in each 7‑day interval using the “average of start/end population” method. Our rates here differ slightly (for the last two) from Jikky’s one who had just done a “back-of-the-napkin” calculation of raw rates to illustrate its point (regrettably left unanswered by the Penn Professor).
[Note that the calculations take these papers at face value, despite the very obvious statistical trickery noted by Reeder9 and Fenton10]
To get a better estimate we break-down how we can calculate the infection rate / person-days among the unvaccinated persons exposed, performing the following (Spreadsheet11):

We therefore have, among the unvaccinated, from December 20, 2020, to February 1, 2021, 6 100 events / 9 141 496 days = 66.7 confirmed infections / 100,000 person-days, over 42 days (R12).
Bar-On 2021 (Dagan’s co-author) from July 30 to August 31, 2021, kindly provides us with the values required to calculate the raw rates in its table 2, and we have 4 439 events / 5 193 825 days = 85.46 confirmed infections / 100,000 person-days among the 2 doses group.
The same goes for Bar-On 2022, from January 10 through March 2, 2022, which provides directly, in its section “Protection Conferred by the Fourth Dose” a raw infection rate among the “Three-dose group” of a whopping 361 cases per 100,000 person-days.
Magen 2022 isn’t so kind to us, and we have, on figure 2, to perform the same estimate than for Dagan 2021, on the recipients of 3 doses.

This results in another huge rate of 347.7 confirmed infections / 100,000 person-days, over 21 days (R13), from January 3 to February 18, 2022, confirming that our method is likely accurate by comparison to the 361 of Bar-On 2022, over the same period.
A revision of the mouse’s plot would therefore result in the following (R14).

We can compare the infection rates at 0 (Dagan 2021), 3 doses (Magen 2022), and the advertised 2 doses vs 3 doses efficacy (Moreira et al., 202215). The latter figures were provided in the Figure 3 “Cumulative Incidence of Covid-19 after a Third Dose of BNT162b2.” an another study reporting on a “randomized clinical trial” commissioned by Pfizer & BioNTech, pulling the traditional “central laboratory” trick16. Impressive efficacy against infection (again):

Yet if we overlay the cumulative incidence curve from the Dagan 2021 study on this graph we start to see the problem - that the vaccinated are performing worse than the original unvaccinated cohort.

Translating the values over the period we care about, from 0 to 42 days, results in the following (accurate) estimates of data we can compare (R17) with our Israeli studies.

We can then compare the cumulative rate of confirmed infections per 100.000 person-days at risks, at 3 doses, in Magen 2022, to the advertised one (R18). The cumulative incidence rate for Bar-On 2021 was calculated using the average proportional incidence rate of Magen and Dagan from days 0 to 28, then extrapolated to the cumulative incidence observed at Day 32.
Really Real World Data?
The following chart therefore compares the Incidence Rates observed in “real life” (according Israel’s own studies) for the “underdog” of each study (dashed) - against Moreira’s advertised results (continuous).
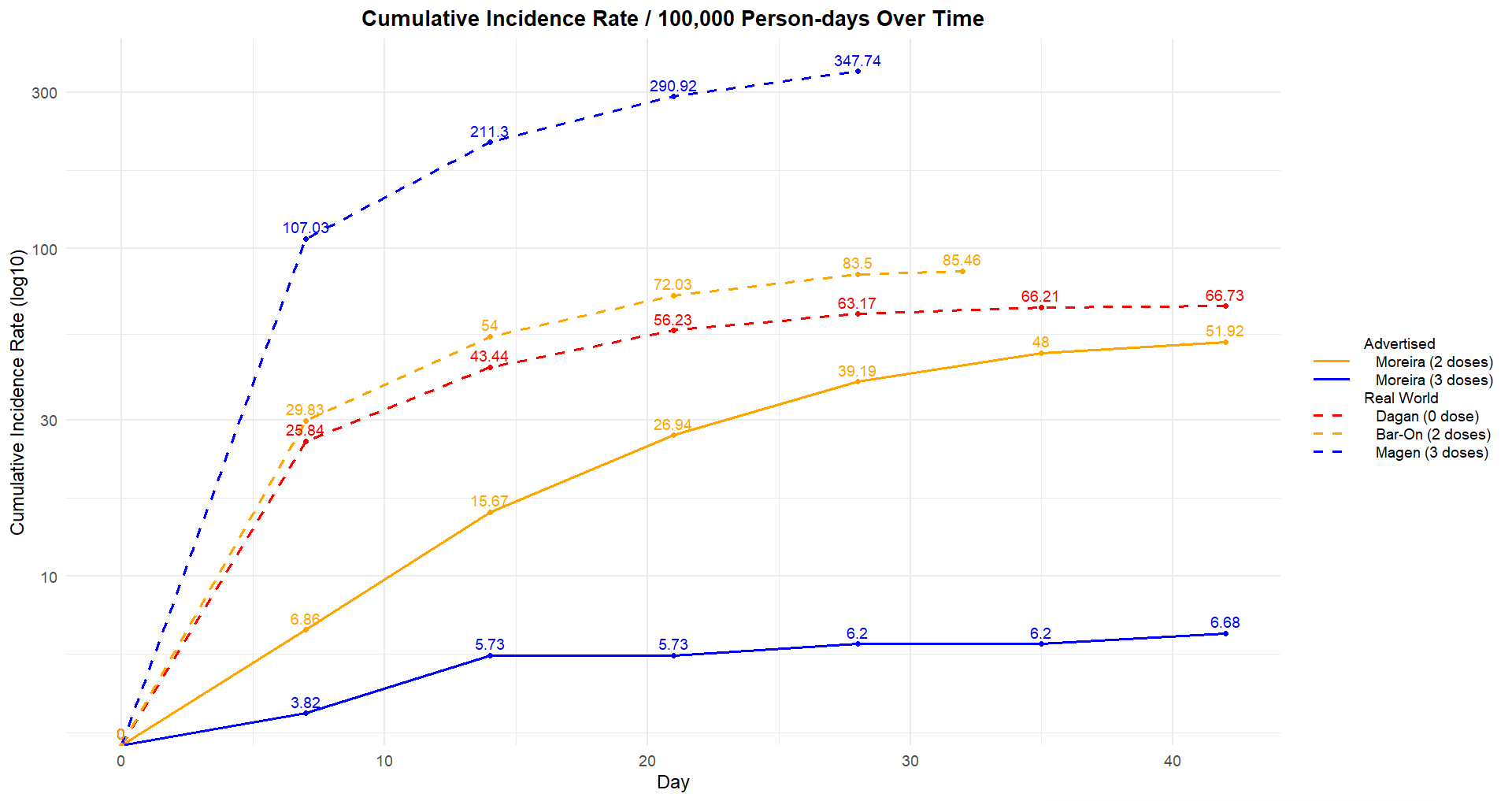
Of course one could argue that the background infection rate19, in Dagan 2021, from December 20, 2020, to February 1, 2021, was lower than the peak observed during Magen 2022, from January 3 to February 18, 2022.

But then, similarly to our introduction’s Australian chart, one would have to explain how this peak of infections occurs in a population of 60+ over 80% vaccinated20…
.. with 3 doses of a vaccine which
was 100% effective in preventing COVID-19 cases21
We’re also still waiting a valid explanation as per why emergency calls for cardiac arrests had increased drastically in Israel during the roll-out of this safe product22, but that’s a question for another day.

Conclusion
Putting this all together it is clear that the big four Israeli studies used to create a false narrative in 2021-2022 that the COVID vaccines were preventing infection falsely represented their own claims.
There never was a beneficial impact on infection rates, and the “real real world data” (released by the UKHSA and NSW health also to prop up that same narrative) had to be pulled (despite attempts to cover up the problem23) when it became too obvious that the vaccinated were becoming more susceptible to COVID with each dose - as perfectly illustrated by the Cleveland Clinic study24 in 2023.
 for study participants stratified by the number of COVID-19 vaccine doses previously received. Day 0 was 12 September 2022, the date the bivalent vaccine was first offered to employees. Point estimates and 95% confidence intervals are jittered along the x-axis to improve visibility.")
Worse still, this whole episode ended up uncovering one of the biggest scandals of this “Real World Data” fiasco - that some or all of that data used may even be synthetic. That, is, not real at all.
Of course we don’t expect you to take our word for it… it’s all explained in last month’s article here:
Meanwhile, Happy New Year to everybody except the data manipulators.
All the scripts & source files used are provided in the following Github repository.

Even simpler than that. When you use relative risk instead of absolute risk, it’s because you know your results are BS.
Another word for data manipulator is criminal.