
Pfizer/BioNTech C4591001 Trial - A few new evidences of Pfraud
Antibodies data reveals more on BNT subjects' COVID cases non-accounted by the testing bias, and on the absence of blinding during the trial

Introduction
It’s been a while since the last publication of a lengthy article on the Pfizer/BioNTech trial - hence, a short recapitulation of situation is in order.
It was already obvious from the start, as established by Christine Cotton’s expertise, that the protocol itself was deeply flawed, in order to produce misleading results in favor of the BNT162b2 product1.
Given:
the numerous elements we had gathered in our 9 minutes recapitulation video, in April2
and the fact, highlighted by the work of Josh Guetzkow & Retsef Levi, recently confirmed by the Daily Clout’s team 33… that the product tested for most subjects (except for 252 Americans) wasn’t even the one distributed to the public4…
… It seems to us that no one can any longer assert, in good faith, the proper testing of the Pfizer-BioNTech product.
Informed consent was simply impossible for the public.
Various legal efforts are ongoing, and we can’t recommend enough to people to support, among others, the fights of Brook Jackson5 in the US, of Andrew Bridgen6 in UK, of Augusto Roux7 in Argentina, of the AMPS8 and Dr Melissa McCann9 in Australia. To quote but a few, and note that we need more of such initiatives.
The main author of this blog - your servitor - has been focused since on presenting these findings in public discussions, with Josh Guetzkow at Rounding The Earth10, with Christine Cotton at Pierre Chaillot’s French “Decoder l’éco”11, and Dr Peter McCullough’s Courageous Discourse12.
Yet, while we wait until the “regulators” take notice and decide to regulate, there are still plenty of areas of shadows worth exploring in this trial… So, back at it.
We’re following up, here, on one of the many precious insights of Twitter’s most famous Mouse - verified by “The Digger”, who was kind enough to provide his Python code, a while ago13.
In this thread, the Mouse analysed the antibodies testing at visit 3, until the November 14 cut-off, and highlighted the fact that it was telling a very different story than the “8 BNT cases - 162 Placebo cases” presented to justify the alleged efficacy, and showing an efficacy post dose 1 of 53% at EUA times.

Two verifications are always better than one ; and if you have set up your project in the way described here14, you can confirm the Mouse’s figures using this short R script.
We already made clear, before, that it was “highly likely” that the efficacy was completely fraudulently manufactured - or at least highly “artificially inflated”, playing on two major fraudulent patterns :
testing the BNT subjects less than Placebo as far as PCRs were concerned15
and deleting subjects producing unwanted results16
We don’t know when subjects have been deleted - nor how many were deleted to manufacture the efficacy illusion, against how many were used to forge the “safety”.
But we should be able to evaluate how many subjects were involved in the “sub-testing bias”, yet weren’t detected by the PCR organized faulty testings.
We can do so by comparing the subjects who received BNT or placebo, and who were or were not detected via PCR analysis, but were later detected through N-antibodies measurements.
Antibodies measurements during the Trial
The antibodies measurements - contrarily to the PCRs on symptomatic visits, were supposed to happen for every subject at visit 1, then 30 days after dose 2. They are allowing us to know who caught COVID between visit 1 and visit 3, and wasn’t detected.
Two categories of antibodies were examined:
Anti-S antibodies detect antibodies that target the spike protein (S) found on the virus's exterior. These antibodies can be identified following both natural infection and vaccination, as COVID ‘vaccines’ are designed around the spike protein. Christine Cotton already reviewed these with us, in an article highlighting another major anomaly on phase 117.
Anti-N antibodies were examined via tests that respond to a molecule within the SARS-CoV-2 virus known as the nucleocapsid (N). Anti-N antibodies are of particular interest, because the only known method for a subject to produce them is through contracting COVID-19.
The N-antibodies were measured during the trial via a mNeonGreen SARS-CoV-2 “Nucleoprotein-Binding Antibodies Assay”18. As the name suggests, this test targets the Nucleoprotein, which is a component of the nucleocapsid1920. It’s worth noting that N-antibodies aren’t a perfect detection method, with 5.5% of the subjects testing negative at 100 days according to observational studies21 (reference kindly provided by
).Antibodies were scheduled to be measured, as summarized in this consent form22, at various steps of the process:
Visit 1 (V1_DAY1_VAX1_L - while receiving dose 1)
Visit 3 (V3_MONTH1_POSTVAX2_L - a month after dose 2, labeled “1 month visit”)
Visit 4 (V4_MONTH6_L - at 6 months)
etc.

If subjects had positive N-antibodies measurements at dose 1, they were therefore considered as having already caught COVID, discarded from the “efficacy population” of the study - and couldn’t be used anymore for the “efficacy analysis”.
If you read, as you should have, the Jikkyleak’s thread above, you’ll also have noted a study on the Moderna product, noting that N-antibodies production, among vaccinated individuals, was 40% to 93% lesser than the one of non vaccinated individuals23.
PCR during the trial
We already extensively developed the subject of the PCR tests in several articles242526, so we won’t spend long detailing this point. Let’s just say PCR testing of symptomatic subjects was the “active measure” aiming to confirm a symptomatic COVID case.
Problematic
We will aim here to isolate Phase 3 subjects, who were negative at visit 1, both in terms of PCR & N-binding test (i.e they received their first dose while they hadn’t COVID), to N-binding Positive at visit 3, and evaluate how many were properly detected by a positive PCR between visit 1 & visit 3, prior March 13, 2021 BLA cut-off27.
Merged & normalized Data
The data is merged and normalized from 3 required .XPT files (ADSL, ADVA, MB28) by the following R script, resulting in a more unified and normalized .CSV file29.
Merging these files results in 220 074 records of N-binding & PCR tests, performed on 46 561 subjects.
Preliminary Exclusions
After excluding 195 Phase 1 subjects, we have 46 366 subjects (23 184 BNT162b2 (30 mcg) & 23 182 Placebo).
15 subject ids have ADRG exceptions documented (6 subjects who registered twice, 3 without CRF vaccine data), and are excluded.
Excluding children under 16-years-old (1131 BNT & 1130 Placebo) brings us to 44 090 subjects.
Two subjects from the placebo group did not have a visit 1 test, and are excluded.
153 BNT & 123 Placebos are missing a “Visit 1” Test (either PCR or NBinding), and aren’t included in this analysis. It’s worth commenting, as it falls just under significance using a chi-square test, and was the occasion to “let in” subjects who may have had already a prior infection (it’s also very possible, given the weak advantage it gave to the BNT group and the lack of statistical significance, that this simply occurred by chance).

Visit 1 Results
21 891 BNT & 21 921 Placebo subjects therefore have known PCR & N-Binding Visit 1 Results.
At visit 1, 687 BNT subjects and 714 Placebo subjects tested positive for COVID either via N-Binding or PCR. 1 BNT & 2 Placebo had at least one undetermined result. 12 BNT & 14 Placebo didn’t receive their first dose. Neither are significant.
21 191 BNT & 21 191 Placebo subjects therefore started with negative PCR & N-Binding Results at visit 1, and received their first dose.
Visit 3 - Attendance
The first new interesting find of this paper comes with “Visit 3” antibodies measurements - which as mentioned above was the “one month post dose 2” antibodies blood test, allowing us to determine if the subject contracted COVID between dose 1, and dose 2 + 30 days.
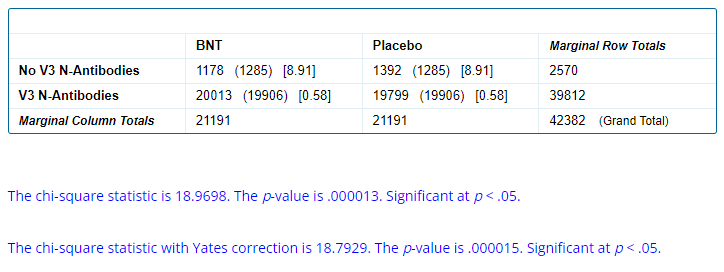
The first problem here is that 1 178 BNT subjects & 1 392 Placebo weren’t tested for V3 Antibodies, which represents a significant statistical difference.
These subjects have been further analysed to detect if a diagnosed COVID could explain this anomaly.
21 of the 1178 missing visit 3 BNTs have a positive central PCR (1.78%), and 105 of the 1392 Placebo subjects missing have a positive PCR (7.5%) (without paying too much attention to the time window as Visit 3 was performed between 46 and 138 days post visit 1…). Detection of COVID appear to have been a factor in subjects not having his scheduled visit 3. But it doesn’t suffice to explain the offset - as even if we exclude these positive PCRs, it remains a significant difference.

The most likely explanation appearing at first sight is that Pfizer/BioNTech didn’t care much to know if their Placebo had developed N-Binding antibodies, it wasn’t qualifying them for efficacy. On the other hand, they may have wanted to have samples on vaccinated people.
In any case, it’s another evidence of major difference of treatment between arms which shouldn’t have happened (and couldn’t have happened by chance) - also called fraudulent unblinding… and a new mystery of tests missing from an arm.

Visit 3 - N-Binding Results
19 928 BNT & 19 511 Placebo were negative on visit 3 N-Binding Antibodies testing, and 85 BNT subjects were positive, against 288 Placebo.
An apparent vaccine efficacy of 71% against infection Post Dose 1 - remarkable increase from the EUA’s 53%.
Keeping in mind that :
N-Binding detection isn’t perfect
the 301 missing subjects unknown
and the “missing tests” which may have been oriented to avoid positive BNT subjects in “non blinded” conditions
So in no case do we express it as an actual efficacy of the product.
What’s more interesting, here, is to observe how many of these 85 BNT & 288 Placebo have been undetected by Central PCR, prior their visit 3.
53 BNT cases were detected via Central PCR, along with 201 Placebo cases.
It leaves us with 32 undetected cases among BNT subjects (37.6% of the 85 cases), compared to 87 undetected cases in the placebo group (30.2%).
This returns a non-statistically significant result on a chi-square test (19.6% chances).

Nevertheless, at global phase 3 > 16 yo scale, subjects in the BNT groups were 7.4% more likely to avoid PCR detection, while having positive COVID specific antibodies 1 month post dose 2.
Undetected Cases by Trial Sites
Going further, as we know by now that the fraudulent patterns are different on each site, we can quickly detect for sites standing out for their exceptional ability not to detect a positive BNT using PCR.
Cases were detected on 94 sites. We only considered sites which had at least 1 detected case in each treatment arm and more than 5 total cases, bringing the total of sites concerned to 12. Among these, 4 (sites 1009, 1093, 1120, 1241) stand out as abnormal, in terms of variations of testing rates between treatment arms, to the benefit of the treatment arm.
Testing variations can be represented in contingency tables - both for “the 90 normal sites” and “the 4 abnormal sites” - in order to evaluate equal treatment between arms for both categories.
Predictably, the result in “normal sites” has no statistical significance (Fisher exact test p-value : 0.58). On the other hand, the testing rates between arms in the 4 abnormal sites is highly significantly different.

Another angle on this data is to compare testing rates between normal sites & abnormal ones.

Obviously, to beat Christine Cotton’s favorite dead horse, the protocol was beyond faulty, and a vast part of the COVID infections went undetected (35%~ of the BNT ones & 32% of the Placebo ones), on “normal” sites.
The 4 sites we are underlining, on the other hand, showed a lot of zeal to detect an awesome 80% of the Placebo COVID infections. Somehow, their BNT went vastly undetected, as they detected only 37.5% of their COVID infections.
So, what’s left ? Ah, yeah. As highlighted by Igor Chudov in a new excellent article30… the market is seeing it too, Albert31.

Open question to researchers
Richard Ward32 recently formulated an interesting hypothesis during our discussion of the trial: “the COVID ‘vaccination’ could reduce viral load in the vicinity of the typically swabbed area, reducing the viral load later detectable by PCR” - which would partially contribute to explain the lack of BNT subjects detection33. As I don’t have the knowledge to answer this question, or evaluate the impact it would potentially have, I would like to collect elements on that. Please comment if you have insights or additional studies on the mater.
Code
The R code employed to generate this analysis can be accessed on GitHub.
Pfizer/BioNTech C4591001 Trial - April 23 - Recapitulation Video

A mouse produced, based on our script, the following video that this Substack accompanies as collection of sources (click here or on the miniature to access it on Rumble). It recapitulates, as shortly as possible, what someone who hasn’t read our past articles and the others we referenced should know about the Pfizer/BioNTech fraudulent trial…
Click the picture to access the tweet.



Pfizer/BioNTech C4591001 Trial - Downloading & Exploiting the XPT Files

This article is boring and contains no cheese - we’re publishing it in order to ease the life of other researchers and document the method of incoming articles. Introduction A few have objected that Perl, (although a fantastic language), wasn’t the most commonly practiced, which wasn’t easing the verification of our arguments by third parties. While in th…
Pfizer/BioNTech C4591001 Trial - Local & Central Testing Rates on Symptomatic Visits, by Trial Sites

This article is the product of a joined effort with Josh Guetzkow. Both authors contributed equally to this paper. Introduction This short article follows up on our analysis of the Local vs Central PCRs performed on symptomatic visits. In this previous post, we demonstrated a significant offset in local testing rates vs central ones overall through the EUA…
Pfizer/BioNTech C4591001 Trial - The 301 Mysteriously Missing Subject IDs Are Cause for Concern

Introduction The software that assigned subject ID numbers for the Pfizer/BioNTech clinical trial generates ID numbers sequentially, which are assigned to volunteers when they are screened for inclusion in the study. We found 301 “gaps” in the subject ID numbers (missing numbers where there should be one), and in more than a few cases multiple sequential…
Pfizer/BioNTech C4591001 Trial - Phase 1 Antibodies. Where haven't they cheated exactly?

This article is the product of another joint effort with Christine Cotton, who made the original discovery of the major issue we highlight here. Both authors contributed equally to this paper. As usual, we must also thanks Geoff Pain for his cautious rereading & precious lights on technicalities.
Pfizer/BioNTech C4591001 Trial - Positive PCRs & Symptomatic Subjects

We, once again, thanks Josh Guetzkow & Geoff Pain , for their precious assistance and key comments, going through this analysis. Arkmedic (whom you can follow on Substack or on Telegram), Jikkyleaks, the DailyClout’s team 3 & Abstractor team, Twitter’s “A Concerned Amyloidosis”
Pfizer/BioNTech C4591001 Trial - How many mathematical proofs of fraud in this trial do we need, for independent inquiries to finally start ...?

Introduction This article is the product of a joined effort with Josh Guetzkow. Both authors contributed equally to this paper. We covered in a previous article how to identify accurately in the PHMPT documents the 372 exclusions labelled “other important protocol deviations”, and why what could seem like a small detail mattered a lot as far as providing …
Pfizer/BioNTech C4591001 Trial - Local & Central Testing Rates on Symptomatic Visits, by Trial Sites
This article is the product of a joined effort with Josh Guetzkow. Both authors contributed equally to this paper. Introduction This short article follows up on our analysis of the Local vs Central PCRs performed on symptomatic visits. In this previous post, we demonstrated a significant offset in local testing rates vs central ones overall through the EUA…
It’s worth noting that 7 Placebo (5 pos to neg, 2 neg to pos) tests & 2 BNT (2 pos to neg, 1 neg to pos) tests (local or central, indistinct from the test used) have conflicting duplicates for the same day / test. The first entry was sustained in these marginal (yet weird) exceptions, considering the question of “how could a contradicting test appear later in the table” was open.

Picture credits to “Charles 5”.
Thanks for a great piece of work.
In response to your question posed near the end, to my mind a likely scenario (which might explain some of the mismatch between the apparent results and “real world” experience) is this:
Sore throat, fever etc (ie “symptoms”) represent a normal immune response to infection.
The injections interfere with the immune response, either generally or specifically in relation to the defence mounted to coronaviruses, to which most would have had some degree of immune memory through previous encounters with other coronaviruses.
So: aberrant immune response -> symptom reduction -> less likely to report -> less likely to test.
Hence it’s possible that at least some of the apparent reduction in infections if defined by (symptoms + PCR) from the injections is essentially illusory as it’s based on a faulty assumption that a reduction in the ordinary symptoms of infection is desirable, clinically relevant, and generalisable to a reduction in more severe symptoms.
One of the many crimes in the assessment of these products was the extrapolation of such clinically irrelevant observations to an assumption that they would prevent infection, transmission and protect against severe disease.
Of course, symptom reduction without viral load reduction (which the above would result in) would create a mass of people who were still infected but with reduced symptoms. This would interfere with evolved behaviour pattern by which sick people stay in bed, lounge around at home, and otherwise avoid other people.
This is consistent with the real world failure of these injections and may also explain (partially at least) why each campaign seemed to induce new waves of infections.
Btw the above would (in my opinion) only contribute partially to the problems with these trials.
I’m not at all diminishing the importance of the various statistical “sieves” applied disproportionately to the 2 groups using inadequate blinding (aka “cheating”).
Excellent work as always. Your ability to see over the hill is greatly appreciated. A true scholar and scientist.